Vesicoureteral Reflux (VUR)
Vesicoureteral reflux (VUR) is a condition where urine flows backward from the bladder into one or both ureters and sometimes up to the kidneys. It’s most common in infants and young children, and a major risk factor for recurrent urinary tract infections (UTIs) and kidney damage.
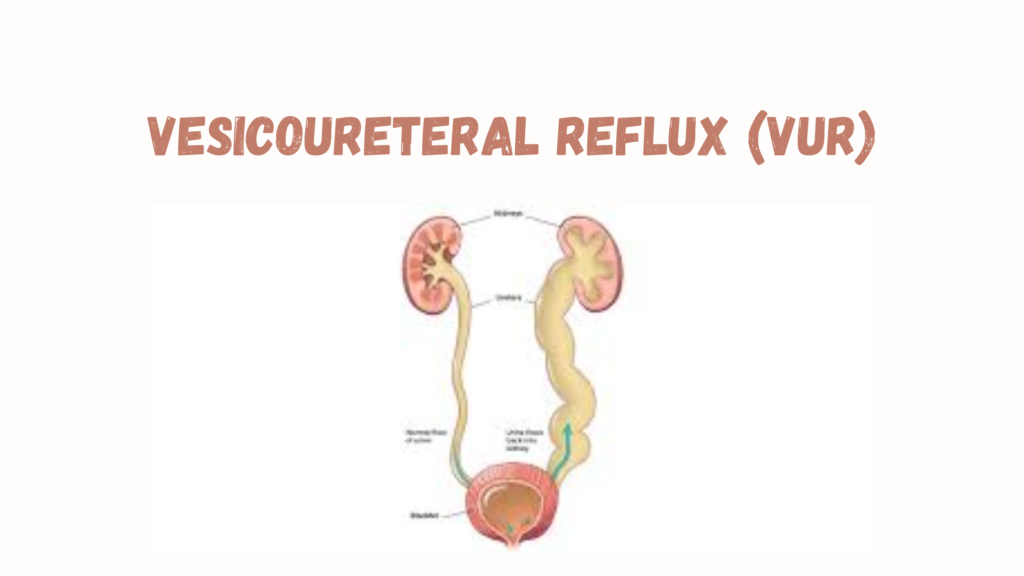
📌 Normal vs. Reflux Mechanism
- Normally, the ureter enters the bladder at an angle, forming a flap-valve that closes during bladder filling and voiding.
- In VUR, this valve mechanism is defective, allowing retrograde flow of urine.
🧬 Types of VUR
1. Primary VUR (most common)
- Congenital defect in the UVJ (ureterovesical junction).
- Often familial (genetic predisposition).
2. Secondary VUR
- Caused by bladder outlet obstruction or high bladder pressure.
- Seen in:
- Posterior urethral valves (boys)
- Neurogenic bladder
- Chronic constipation
🎯 Grading of VUR (I–V)
| Grade | Description |
|---|---|
| I | Reflux into ureter only |
| II | Reflux into ureter, pelvis, and calyces |
| III | Mild to moderate dilation of ureter/pelvis |
| IV | Moderate dilation and tortuosity |
| V | Severe dilation, tortuosity, loss of calyceal detail |
⚠️ Symptoms
- Recurrent febrile UTIs (most common presentation)
- Enuresis (bedwetting)
- Flank or abdominal pain
- Failure to thrive (in infants)
- Hypertension or signs of chronic kidney disease (in severe or long-standing cases)
🧪 Diagnosis
1. Voiding Cystourethrogram (VCUG)
- Gold standard test
- Involves filling the bladder with contrast and watching for reflux during urination
2. Renal Ultrasound
- Looks for hydronephrosis, scarring, or asymmetry
3. DMSA Scan (nuclear medicine)
- Assesses kidney scarring and differential function
4. Urinalysis and Culture
- Recurrent UTIs are the main clue
🩺 Treatment
Depends on:
- Age
- Severity (grade of VUR)
- Frequency of UTIs
- Kidney function and scarring
Non-Surgical (Conservative) Management
- Often used in low-grade (I–III) reflux
- Prophylactic antibiotics to prevent UTIs (e.g., low-dose TMP-SMX or nitrofurantoin)
- Watchful waiting with regular imaging
- High rates of spontaneous resolution, especially in young children
Surgical or Procedural Treatment
- Indicated for:
- High-grade reflux (IV–V)
- Recurrent febrile UTIs despite prophylaxis
- Renal scarring or deterioration
- Non-resolution over time
Options:
- Endoscopic injection (Deflux®)
- Gel injected into UVJ to improve valve function
- Minimally invasive, outpatient
- Ureteral reimplantation surgery
- Reconstructs UVJ to prevent reflux
- Very effective but more invasive
🔄 Prognosis
- Excellent in most children, especially with early detection and proper management.
- Long-term follow-up needed to monitor for:
- Renal scarring
- Blood pressure issues
- Renal growth