Tropical sprue is a chronic malabsorption syndrome seen in individuals living in or visiting tropical and subtropical regions. It is characterized by chronic diarrhea, nutrient malabsorption, and villous atrophy of the small intestine—similar in appearance to celiac disease, but with a different cause and treatment.
🌍 Epidemiology
Endemic in parts of South and Southeast Asia, the Caribbean, Central and South America.
Affects both locals and long-term visitors (e.g., missionaries, Peace Corps workers).
More common in adults, but can affect all ages.
🧬 Pathophysiology
Exact cause unknown, but likely related to:
Chronic intestinal infection (possibly bacterial overgrowth with enterotoxigenic organisms)
Damage to small intestinal mucosa → villous atrophy, enzyme deficiency, and malabsorption
Malabsorption mainly affects folate, vitamin B12, and fat-soluble vitamins.
😖 Symptoms
GI Symptoms
Nutritional Deficiency Symptoms
Chronic diarrhea
Fatigue
Steatorrhea (fatty stool)
Weight loss
Bloating and gas
Glossitis, stomatitis
Abdominal cramping
Peripheral neuropathy (B12 def.)
Nausea
Anemia (macrocytic or mixed)
🧪 Diagnosis
🔬 Laboratory Tests
Macrocytic anemia (low B12 and folate)
Low albumin, calcium, and other micronutrients
Stool fat test: confirms fat malabsorption
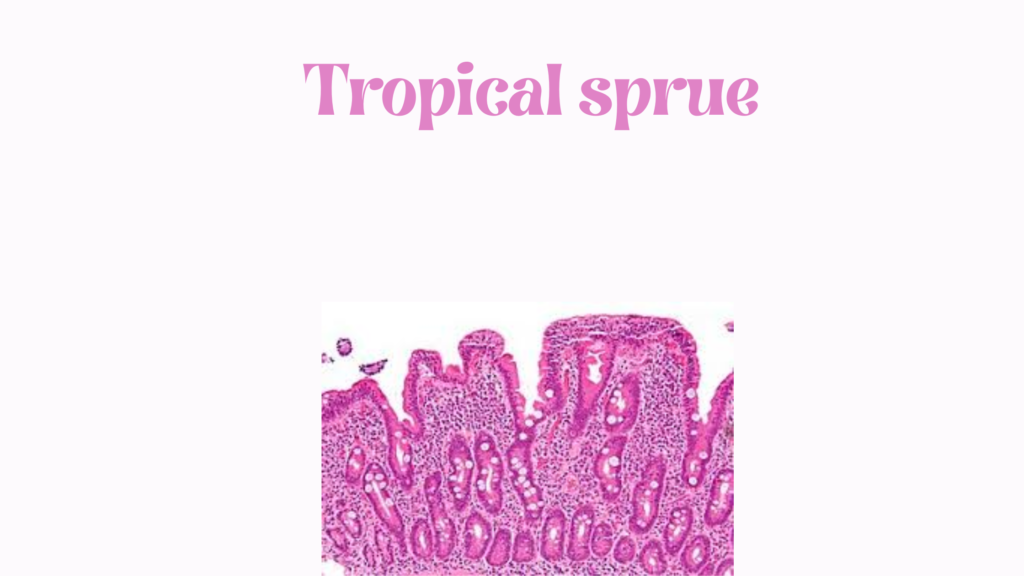
🧫 Small Bowel Biopsy
Shows villous atrophy, crypt hyperplasia, and increased inflammatory cells
Looks similar to celiac disease, but celiac serologies are negative
🌬️ D-xylose test or lactose breath test
May show carbohydrate malabsorption
❗ Differential Diagnosis
Condition
Key Differentiators
Celiac disease
Positive tTG or EMA antibodies; gluten-sensitive
Whipple disease
PAS-positive macrophages, systemic symptoms
Crohn’s disease
Skip lesions, transmural inflammation
Giardiasis
Protozoal infection; diagnosed via stool O&P
SIBO
Positive breath test, usually no villous atrophy
💊 Treatment
✅ Antibiotics
Tetracycline 250–500 mg orally 4× daily for 3–6 months
Alternative: Doxycycline for better tolerability
✅ Nutritional Replacement
Folic acid 5 mg/day (often leads to rapid clinical improvement)
Vitamin B12 (IM injections or oral if mild)
Replenish iron, calcium, magnesium, zinc, and fat-soluble vitamins as needed
✅ Supportive Care
High-calorie, nutrient-rich diet
Avoid raw or contaminated foods in endemic areas
📉 Prognosis
Excellent with treatment.
Most patients show rapid improvement within weeks.
If untreated, can lead to severe malnutrition and long-term GI damage.