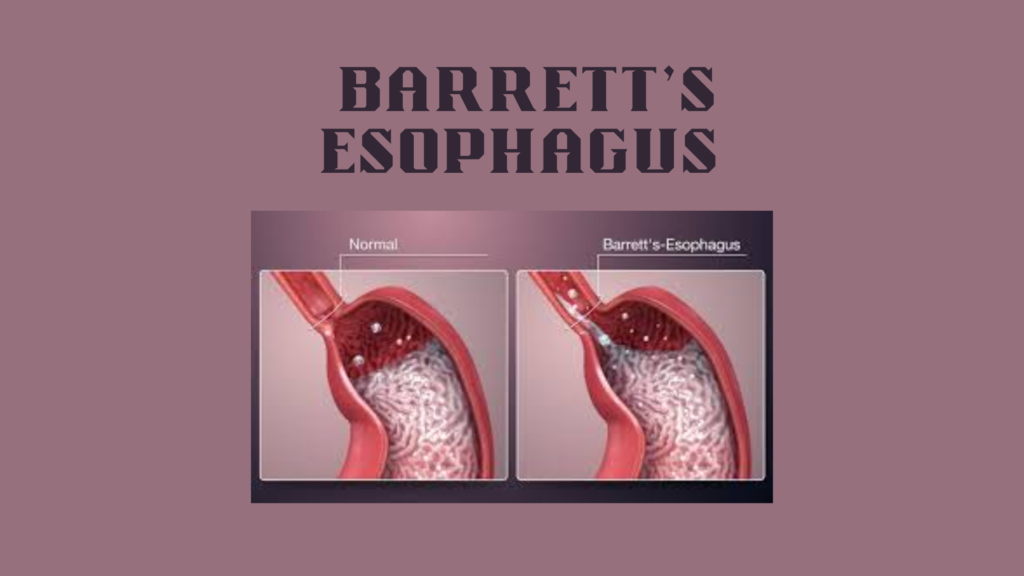
Barrett’s esophagus is a condition in which the normal squamous cells lining the lower esophagus are replaced by columnar cells (like those in the intestines) due to chronic acid exposure—usually from gastroesophageal reflux disease (GERD).
This change is called intestinal metaplasia, and it’s significant because it increases the risk of esophageal adenocarcinoma, a type of esophageal cancer.
🧬 Pathophysiology
Chronic acid reflux → injury to esophageal lining
Body responds by replacing squamous cells with acid-resistant columnar cells
These intestinal-type cells are not supposed to be in the esophagus
Over time, this metaplasia can progress to dysplasia, then cancer in rare cases
⚠️ Risk Factors
Risk Factor
Details
Chronic GERD
Most important risk factor
Male gender
2–3x more common in men
Age >50
Higher risk with age
White race
Most common in Caucasians
Obesity
Especially central (abdominal) obesity
Smoking history
Increases risk
Family history
Possible genetic link
😖 Symptoms
Often asymptomatic or symptoms overlap with GERD:
Chronic heartburn
Regurgitation
Difficulty swallowing (dysphagia)
Chest discomfort
No specific symptoms due to Barrett’s itself
🧪 Diagnosis
🩺 Upper Endoscopy (EGD):
Visualizes the salmon-pink mucosa (normal esophagus appears pale)
Biopsy required to confirm intestinal metaplasia
🧫 Histological Confirmation:
Presence of goblet cells (seen with special stains) confirms Barrett’s
🧪 Classifying Dysplasia (if present)
Stage
Risk Level
No dysplasia
Low cancer risk
Low-grade dysplasia (LGD)
Moderate risk, requires close follow-up
High-grade dysplasia (HGD)
High risk of progression to cancer
💊 Management
✅ If No Dysplasia:
Long-term proton pump inhibitors (PPIs) to suppress acid