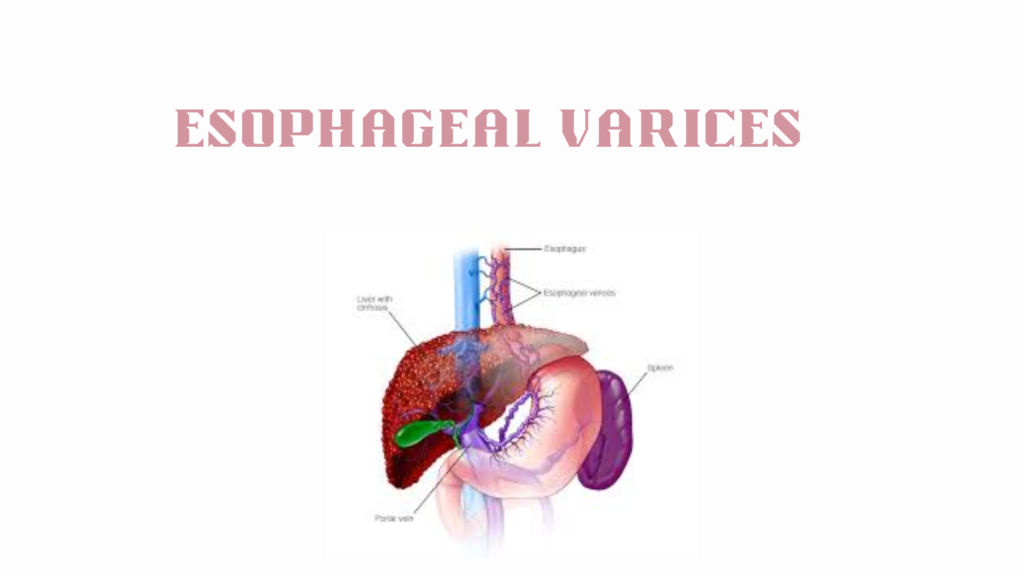
Esophageal varices are dilated veins in the lower part of the esophagus, most commonly caused by portal hypertension, typically due to liver cirrhosis. These veins are fragile and can rupture, leading to life-threatening bleeding.
🧬 Pathophysiology
Portal hypertension (increased pressure in the portal vein) causes blood to reroute through smaller veins like those in the esophagus.
These veins dilate abnormally under pressure.
Over time, they become thin-walled and fragile, prone to rupture and massive hemorrhage.
⚠️ Risk Factors for Bleeding
Risk Factor
Explanation
Large varices
Wider diameter → more tension
High portal pressure
Hepatic venous pressure gradient > 12 mmHg
Red wale marks (on endoscopy)
Indicative of imminent rupture
Severe liver disease
High MELD/Child-Pugh scores
Active alcohol use
Worsens portal pressure and coagulopathy
Previous variceal bleed
High recurrence risk
😖 Symptoms
Varices themselves are asymptomatic until they bleed:
⚠️ Signs of Bleeding:
Hematemesis (vomiting blood)
Melena (black, tarry stools)
Hematochezia (bright red blood per rectum—if brisk bleeding)
Lightheadedness or syncope
Signs of shock: low BP, rapid heart rate, cold extremities
🧪 Diagnosis
🔬 Upper Endoscopy (EGD) – gold standard
Identifies and grades varices (small, medium, large)
Looks for signs of high bleeding risk (red spots, cherry red marks)
Used to screen cirrhotic patients
🧫 Other Workup:
CBC: anemia, thrombocytopenia
LFTs: underlying liver disease
Coagulation panel: INR, PT/INR elevated in liver failure
Ultrasound with Doppler: assess portal vein, liver architecture
🩺 Management
✅ Prevention (in known cirrhotics)
Approach
Details
Endoscopic screening
At diagnosis and intervals thereafter
Non-selective beta-blockers
Propranolol or nadolol to reduce portal pressure
Endoscopic variceal ligation (EVL)
Banding varices if high-risk or intolerant to meds
🚨 Acute Bleed: Medical Emergency
Step
Details
IV fluids and blood
Cautious resuscitation (avoid over-transfusion)
Vasoactive meds
Octreotide or terlipressin
Antibiotics
Ceftriaxone to prevent infection (common trigger)
Urgent endoscopy
Band ligation or sclerotherapy
Balloon tamponade (Sengstaken-Blakemore tube)
Temporary measure if bleeding uncontrollable
TIPS procedure
Transjugular Intrahepatic Portosystemic Shunt for recurrent/refractory bleeding
💊 Long-Term Management (After Bleed)
Repeat EVL every few weeks until varices are obliterated
Continue beta-blockers
Evaluate for liver transplant if cirrhosis is advanced