Esophageal stricture refers to an abnormal narrowing of the esophagus, which can cause difficulty swallowing (dysphagia), food impaction, and sometimes chest discomfort. It is often a complication of chronic reflux (GERD) but can have various other causes.
🧬 Types of Esophageal Strictures
🔹 Benign Strictures (most common)
Result from chronic inflammation and scarring
Causes:
GERD-related peptic stricture
Post-surgical or radiation injury
Caustic ingestion (e.g., lye, bleach)
Eosinophilic esophagitis
Infections (especially in immunocompromised patients)
Post-endoscopic procedures (e.g., after EMR or ablation)
🔹 Malignant Strictures
Caused by esophageal cancer
Often progressive, associated with weight loss and pain
⚠️ Symptoms
Symptom
Description
Dysphagia
Trouble swallowing solids, then liquids
Food impaction
Sensation of food “sticking”
Regurgitation
Of undigested food or saliva
Heartburn
Often present with GERD-related strictures
Chest pain
Especially with eating
Weight loss
In severe or cancer-related cases
🧪 Diagnosis
🔬 Upper Endoscopy (EGD)
Best test for evaluating and treating strictures
Direct visualization of the narrowing
Biopsies to rule out cancer or eosinophilic esophagitis
🧪 Barium Swallow (Esophagram)
Shows location, length, and degree of narrowing
Useful before dilation to assess for perforation risk
💊 Treatment
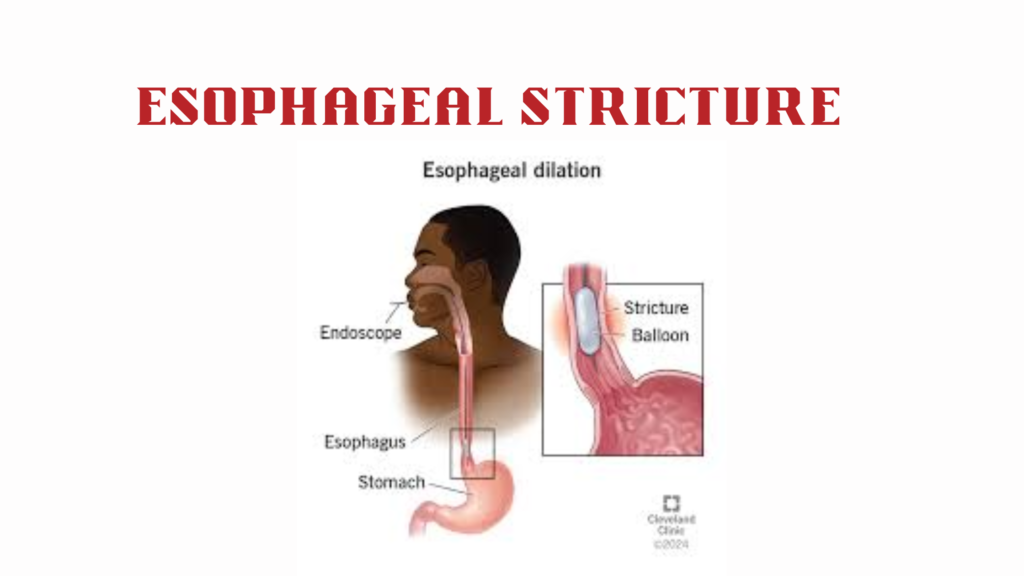
🔹 Endoscopic Dilation (Mainstay)
Balloon or bougie dilators to stretch the narrowed segment
May need repeated sessions
🔹 PPI Therapy
Long-term proton pump inhibitors to reduce acid and prevent recurrence (especially for peptic strictures)
🔹 Steroid Injections
Into stricture site in refractory cases (e.g., eosinophilic esophagitis)
🔹 Stent Placement
For refractory benign strictures or palliative care in malignant cases
🔹 Surgery
Rare; used for severe, complex, or caustic strictures not responding to dilation
📉 Complications
Recurrence (common, especially if GERD not controlled)
Bleeding or esophageal perforation (rare but serious dilation risk)