Achalasia is a rare, chronic esophageal motility disorder where the lower esophageal sphincter (LES) fails to relax properly, and the esophageal muscles lose coordinated movement. This leads to difficulty swallowing (dysphagia), regurgitation, and sometimes chest pain or weight loss.
🧬 Pathophysiology
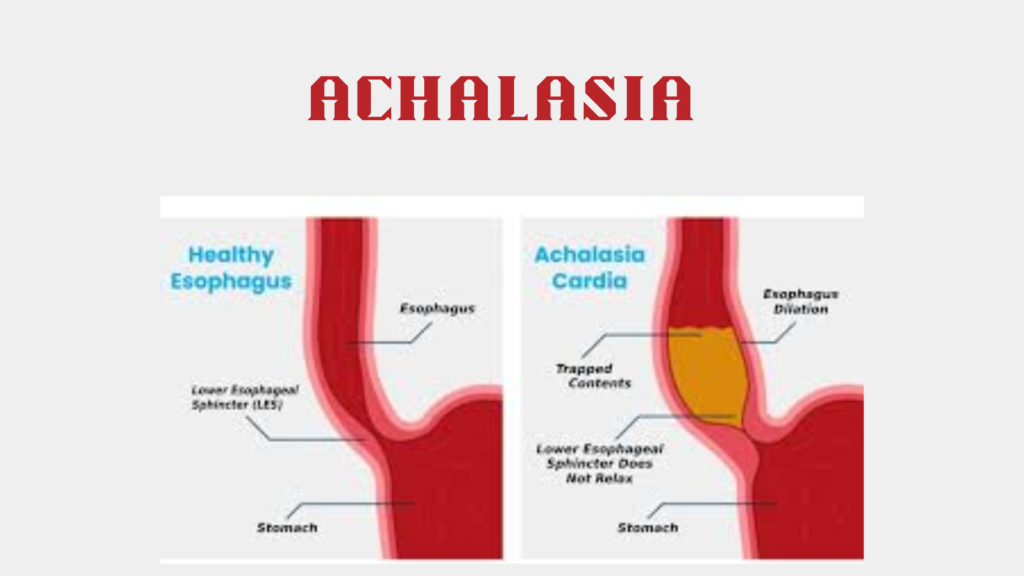
- The esophagus loses peristalsis (wave-like muscle contractions that move food down).
- The LES remains abnormally tight, preventing food from entering the stomach.
- Over time, the esophagus may dilate and become functionally ineffective.
🔍 Cause:
- Typically idiopathic (unknown cause), but thought to involve degeneration of nerve cells (myenteric plexus).
- Rarely associated with infections (e.g., Chagas disease – Trypanosoma cruzi), autoimmune conditions, or malignancy.
😖 Symptoms
| Symptom | Description |
|---|---|
| Dysphagia | Difficulty swallowing solids and liquids |
| Regurgitation | Undigested food or saliva |
| Chest pain | Often with meals; may mimic angina |
| Heartburn | Not true reflux, but food retention |
| Weight loss | Due to eating difficulty |
| Coughing at night | Risk of aspiration |
🧪 Diagnosis
1. Barium Swallow Study (Esophagram)
- Shows “bird-beak” appearance: narrowed LES with dilated esophagus above it
2. Esophageal Manometry (Gold Standard)
- Measures pressure in the esophagus
- Findings:
- Absent peristalsis
- Incomplete LES relaxation
- Increased LES resting pressure
3. Upper Endoscopy (EGD)
- To rule out cancer, strictures, or mechanical obstruction
- May show retained food or secretions
📊 Types of Achalasia (Chicago Classification v4.0)
| Type | Manometric Pattern |
|---|---|
| Type I (classic) | Minimal contraction (no pressurization) |
| Type II | Pan-esophageal pressurization (best prognosis) |
| Type III (spastic) | Premature, spastic contractions (worst prognosis) |
💊 Treatment Options
Achalasia is not curable, but symptoms can be managed effectively.
🔹 Non-Surgical
- Pneumatic dilation (balloon stretches the LES)
- Botulinum toxin (Botox) injections into LES (temporary, often for frail patients)
- Medications:
- Nitrates or calcium channel blockers (limited efficacy, short-term use)
🔹 Surgical
- Heller Myotomy (Laparoscopic)
- Cuts LES muscle fibers to relieve obstruction
- Often combined with partial fundoplication to prevent reflux
- Peroral Endoscopic Myotomy (POEM)
- Minimally invasive endoscopic technique
- Effective even in Type III (spastic achalasia)
⚠️ Complications if Untreated
- Progressive esophageal dilation (megaesophagus)
- Aspiration pneumonia
- Malnutrition
- Slightly increased risk of esophageal squamous cell carcinoma
🔄 Achalasia vs GERD
| Feature | Achalasia | GERD |
|---|---|---|
| Swallowing difficulty | With solids and liquids | Rare; usually solids only |
| Regurgitation | Undigested food, esp. at night | Acidic fluid |
| LES function | Fails to relax | Becomes too relaxed |
| Risk of cancer | Squamous cell carcinoma | Adenocarcinoma (via Barrett’s) |
🛡️ Prognosis
- Excellent symptom relief with POEM or Heller myotomy
- Lifelong monitoring may be needed
- No therapy restores normal peristalsis, but relieving LES obstruction improves quality of life